The question of whether a teacher can give a student Advil or any other medication is a complex and sensitive issue that involves legal, ethical, and health considerations. Schools typically have strict policies regarding the administration of medication to students, often requiring written parental consent and specific guidelines to ensure safety. Teachers are generally not authorized to provide over-the-counter medications like Advil unless they have explicit permission and follow established protocols. This is to protect both the student’s well-being and the teacher from potential liability. Instead, educators are encouraged to contact parents or school nurses when a student reports pain or discomfort, ensuring proper care is provided by authorized personnel.
Explore related products






What You'll Learn
![]()
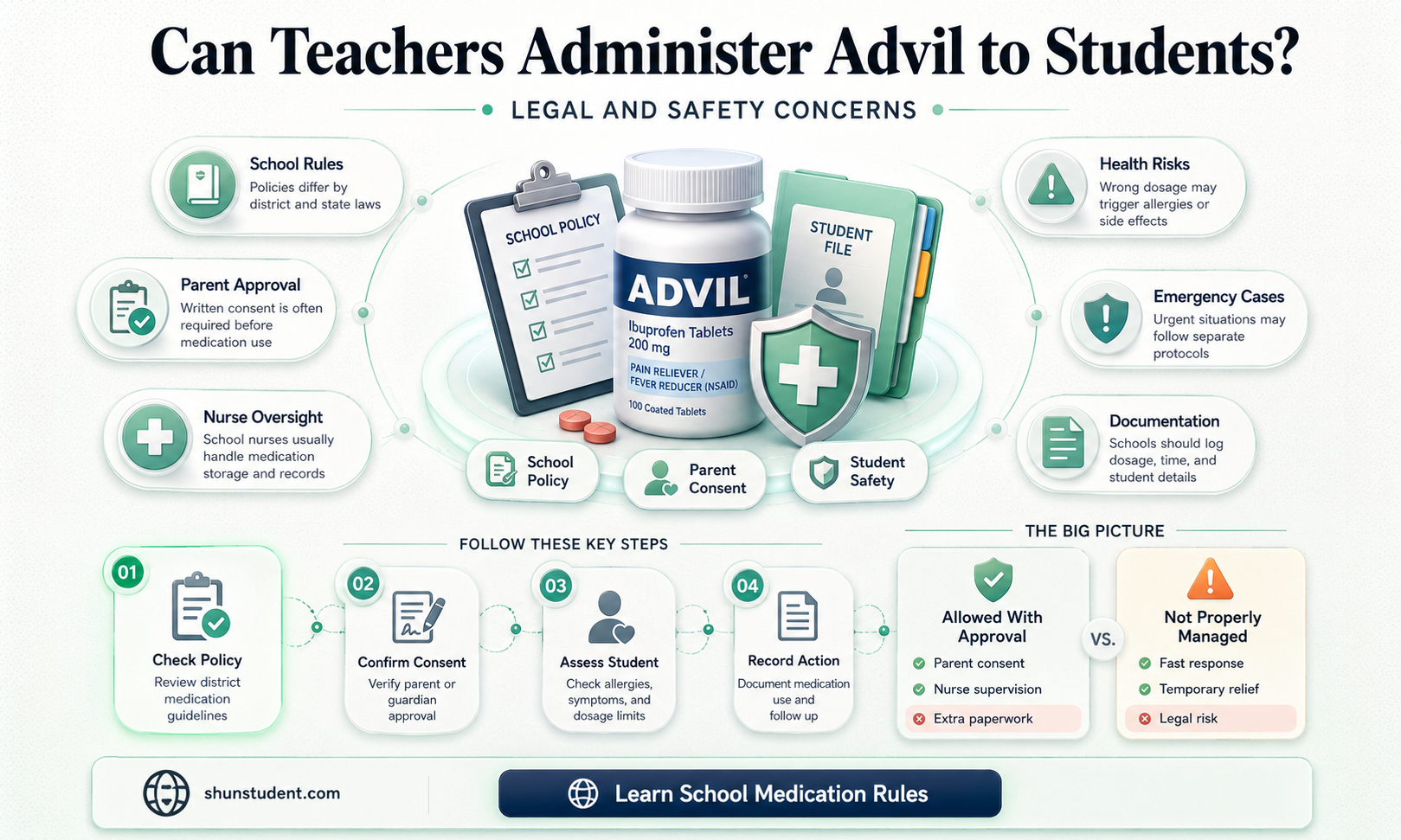
School policies on medication administration
Schools universally mandate that only authorized personnel, typically trained school nurses or administrators, can administer medication to students. Teachers, despite their proximity to students, are generally prohibited from dispensing any medication, including over-the-counter drugs like Advil. This policy stems from liability concerns, potential allergic reactions, and the need for precise dosage control. For instance, Advil (ibuprofen) dosages vary by age and weight: children under 12 typically require 5–10 mg per kilogram every 6–8 hours, while adolescents may need up to 400–600 mg per dose. Without medical training, teachers risk administering incorrect amounts, leading to adverse effects like stomach bleeding or kidney issues.
To navigate this, schools require parents to complete detailed medication authorization forms, specifying dosage, frequency, and duration. These forms must be accompanied by a physician’s prescription, even for OTC medications. For example, a student with chronic headaches might have a form authorizing the school nurse to give 200 mg of Advil every 6 hours as needed. Schools often store medications in locked cabinets, with strict protocols for logging each administration. Teachers play a supportive role by monitoring students for symptoms and alerting the nurse, but they are not permitted to intervene directly.
A comparative analysis reveals that policies vary by state and district. Some schools allow teachers to administer epinephrine auto-injectors (EpiPens) in emergencies, but this requires specialized training and explicit parental consent. In contrast, Advil administration remains strictly off-limits due to its non-life-threatening nature. For example, California’s Education Code (§49423) permits trained staff to administer emergency medications but excludes OTC pain relievers unless prescribed. This highlights the distinction between urgent and routine medication needs.
Practical tips for parents include providing pre-measured doses in labeled containers and ensuring the school has updated contact information for emergencies. Teachers can assist by familiarizing themselves with school policies and encouraging students to carry medical alert cards if they have known sensitivities. While these measures may seem rigid, they prioritize student safety and reduce legal risks for educators. Ultimately, adherence to medication administration policies fosters a secure learning environment while respecting professional boundaries.
Empowering Learners: Student-Led Teaching with a Lesson Rubric Guide
You may want to see also
Explore related products





![]()
Parental consent requirements for giving students medicine
Teachers often face dilemmas when students request over-the-counter medications like Advil for headaches or cramps. In most U.S. states, educators cannot administer any medication, including Advil, without explicit written parental consent. This requirement stems from liability concerns and the potential for adverse reactions, even with seemingly harmless drugs. For instance, Advil (ibuprofen) can cause stomach bleeding or allergic reactions in some individuals, making it crucial to verify dosage history and medical conditions. Schools typically require parents to complete a medication authorization form, specifying the dosage (e.g., 200–400 mg for children over 12) and frequency, often accompanied by a physician’s note for ongoing conditions. Without this documentation, teachers must refrain from providing medication, even if the student appears in distress.
The process for obtaining parental consent varies by jurisdiction but generally involves clear, written permission. Some states allow verbal consent in emergencies, but this is rare and often followed by written confirmation. For example, California’s Education Code mandates that parents provide detailed instructions for any medication, including over-the-counter drugs. Schools may also require medications to be stored in the original container, labeled with the student’s name, and kept in a secure location, such as the nurse’s office. Teachers should never carry or distribute medication unless explicitly authorized by school policy and parental consent. This structured approach ensures accountability and minimizes risks, though it can delay relief for students in need.
Critics argue that strict consent requirements can leave students suffering unnecessarily, particularly in cases of sudden headaches or menstrual pain. However, proponents emphasize that these rules protect both students and educators. For instance, a teacher who administers Advil without consent could face legal repercussions if the student has an undiagnosed kidney condition or is already taking a conflicting medication. To balance these concerns, some schools implement self-carry policies for older students, allowing them to keep approved medications (like Advil) in their possession with parental and medical approval. This approach empowers students while maintaining oversight, though it may not be suitable for younger age groups.
Practical tips for navigating parental consent include maintaining open communication with parents and providing them with clear, concise forms to complete. Schools can also educate families about the risks of over-the-counter medications and encourage them to plan ahead for recurring needs. For example, if a student frequently requires Advil for migraines, parents can pre-authorize its use for the school year, specifying dosages (e.g., 200 mg every 6 hours) and expiration dates. Teachers should familiarize themselves with their district’s policies and avoid making exceptions, even in seemingly minor cases. While these requirements may seem burdensome, they ultimately prioritize student safety and legal compliance.
Effective Strategies for Teaching Students with Autism in the Classroom
You may want to see also
Explore related products






![]()
Legal liabilities for teachers providing medication
Teachers face significant legal risks when administering medication like Advil to students, primarily due to liability concerns and strict regulations. Most schools require written parental consent and a physician’s order for any medication, even over-the-counter options. Without these, a teacher could be held liable for medical complications, such as allergic reactions or overdoses, which can occur even with seemingly safe medications. For instance, Advil (ibuprofen) can cause stomach bleeding or kidney issues in certain individuals, especially if dosages exceed 400–600 mg every 4–6 hours for children over 6 years old. Teachers must understand that good intentions do not shield them from legal consequences if protocols are bypassed.
Consider the scenario where a student complains of a headache, and a teacher offers Advil from their personal supply. If the student has an undiagnosed allergy or interacts negatively with another medication, the teacher could face a negligence lawsuit. Schools often have designated staff, such as nurses, trained to administer medication, and teachers stepping outside their role can void institutional protections. Even in emergencies, teachers should prioritize contacting medical professionals or following district-specific emergency protocols rather than acting independently. The legal principle here is clear: unauthorized medication administration can lead to civil liability and, in extreme cases, criminal charges.
To mitigate risks, teachers should familiarize themselves with their school’s medication policies and state laws. For example, some states allow teachers to administer epinephrine auto-injectors in anaphylaxis emergencies, but only after completing specific training. Similarly, while Advil is accessible, its administration should align with age-appropriate dosages—typically 5–10 mg per kilogram of body weight for children, with a maximum daily limit of 40 mg/kg. Teachers should never estimate dosages or rely on student self-reporting. Instead, they should encourage students to carry their own medication, provided it’s stored securely and disclosed to school authorities.
A comparative analysis reveals that legal liabilities vary by jurisdiction. In some regions, teachers may administer medication in emergencies if they’ve completed certified training, while others strictly prohibit non-medical staff from handling medication. For instance, California permits trained school employees to administer certain medications, but only after obtaining parental consent and a healthcare provider’s written authorization. In contrast, Texas requires a licensed nurse or trained personnel to administer any medication. Teachers must therefore research local laws to avoid inadvertently violating regulations.
Ultimately, the safest approach is for teachers to refrain from providing medication like Advil unless explicitly authorized. Instead, they should focus on creating a supportive environment by ensuring students have access to school nurses or healthcare resources. Practical tips include keeping a list of students with known medical conditions, maintaining open communication with parents, and advocating for comprehensive school health policies. By adhering to legal boundaries, teachers protect both themselves and their students from unnecessary harm.
Empowering Special Needs Students: Strategies for Teachers to Foster Inclusion
You may want to see also
Explore related products






![]()
Alternatives to teachers giving students Advil
Teachers often face the dilemma of whether to administer medication like Advil to students in pain. However, legal and safety concerns make this a risky practice. Instead, educators can adopt alternative strategies to support students while adhering to professional boundaries. One effective approach is to establish a clear protocol for handling student ailments, emphasizing communication with parents or guardians. For instance, if a student complains of a headache, the teacher can contact the parent to inquire about approved medications the student can take at home. This ensures the student receives appropriate care without the teacher assuming medical responsibility.
Another practical alternative is to stock the school clinic or nurse’s office with approved, non-medicated remedies. Items like cold compresses, heating pads, or hydration stations can provide temporary relief for common issues like headaches or muscle aches. For example, a student with a mild headache could be directed to the clinic for a cold compress and a glass of water, which often alleviates symptoms without medication. Schools can also invest in training staff to recognize when symptoms require immediate medical attention, ensuring students get the care they need without overstepping boundaries.
From a preventive standpoint, educators can promote healthy habits that reduce the need for pain relief. Encouraging students to carry reusable water bottles, take breaks during prolonged activities, and maintain proper posture can minimize headaches and muscle strain. For younger students, incorporating short stretching or mindfulness exercises into the daily routine can help prevent discomfort. For instance, a 5-minute desk stretch or deep breathing exercise can relieve tension and improve focus, reducing the likelihood of students needing pain relief during the day.
Finally, schools can implement policies that empower students to manage their own minor ailments within reason. For older students, allowing them to keep approved, pre-labeled medications in the nurse’s office or their backpacks (with parental consent) can provide autonomy while ensuring safety. For example, a high school student with a known history of migraines could keep a single dose of ibuprofen (200–400 mg, as per age-appropriate guidelines) in a sealed, labeled container, accessible only with nurse approval. This approach balances student needs with legal and safety considerations, offering a practical alternative to teachers administering medication directly.
Student Teaching on Reservations: Opportunities, Challenges, and Cultural Insights
You may want to see also
Explore related products






![]()
Emergency situations and medication protocols in schools
In emergency situations, schools must navigate a delicate balance between providing immediate care and adhering to strict medication protocols. A student suddenly develops a severe headache or experiences menstrual cramps during class—can a teacher administer Advil? The answer is almost universally no, due to liability concerns and legal restrictions. Instead, schools typically require written parental consent and a physician’s order for any medication, including over-the-counter drugs like ibuprofen. These protocols are designed to protect both the student and the educator, ensuring that only authorized individuals handle medication and that dosages are accurate. For instance, the recommended dose of Advil for children ages 6–11 is 150–250 mg every 6–8 hours, but this must be verified by a healthcare professional and documented in the student’s file.
Consider the logistical challenges of implementing medication protocols during emergencies. Schools often designate trained staff, such as school nurses, to administer medication, but what happens when a nurse is unavailable? Some states allow schools to train specific employees to handle emergency medications, but this requires additional certification and strict adherence to guidelines. For example, in California, non-medical school personnel can administer medication if they complete a training program and follow a physician’s written instructions. However, this does not typically extend to over-the-counter pain relievers like Advil unless explicitly authorized. Teachers, therefore, are generally instructed to contact the school nurse or emergency services rather than intervene directly with medication.
From a persuasive standpoint, schools should prioritize transparency and education around medication protocols to empower both staff and parents. Clear communication about what constitutes an emergency, how to access medication, and who is authorized to administer it can reduce confusion and ensure swift action when needed. For instance, schools could provide parents with a checklist during enrollment, outlining the steps required to authorize medication for their child, including over-the-counter drugs. Similarly, staff training should emphasize the importance of following protocols, even in urgent situations, to avoid legal and safety risks. By fostering a culture of preparedness, schools can better manage emergencies without compromising care.
Comparatively, medication protocols in schools differ significantly from those in homes or even camps, where flexibility often outweighs formal procedures. At home, a parent might quickly give a child Advil for a fever without hesitation. In contrast, schools operate within a framework of liability and accountability, necessitating stricter measures. For example, while a camp counselor might carry a first-aid kit with ibuprofen for minor injuries, schools rarely allow teachers to keep or distribute such medications without explicit authorization. This disparity highlights the need for schools to strike a balance between rigidity and responsiveness, ensuring that protocols do not hinder timely care in genuine emergencies.
Finally, a descriptive approach reveals the human element behind these protocols. Imagine a teacher witnessing a student in pain, knowing Advil could provide relief, yet being unable to act due to school policy. This scenario underscores the emotional tension educators face when adhering to rules that may seem overly cautious. However, it also reinforces the rationale behind such protocols: protecting students from potential allergic reactions, incorrect dosages, or unauthorized access to medication. By understanding the broader implications, teachers can advocate for system improvements, such as faster access to school nurses or clearer emergency guidelines, while still respecting established procedures. In emergencies, every second counts, but so does every safeguard.
Effective Communication Strategies for Engaging Muslim Parents, Teachers, and Students
You may want to see also
Frequently asked questions
No, teachers should not administer Advil or any medication to students without explicit written parental consent and adherence to school policies.
The teacher should refer the student to the school nurse or administrator, who can follow proper protocols for medication administration.
No, teachers should not keep or distribute medication like Advil in the classroom. All medication should be handled by the school nurse or designated staff.
Administering medication without proper authorization can lead to legal liability, including potential lawsuits for negligence or harm caused to the student. Always follow school and district policies.



![Tumaz Wobble Cushion - Wiggle Seat to Improve Sitting Posture & Stay Focused for Sensory Kids, Balance Disc to Core Strength & Flexible Seating [Extra Thick Balance Board, Pump Included Wobble Board]](https://m.media-amazon.com/images/I/71V7qUV-4HS._AC_UL320_.jpg)