Teaching valvular diseases to nursing students requires a structured, multidisciplinary approach that integrates theoretical knowledge with practical clinical skills. Begin by establishing a foundational understanding of cardiac anatomy and physiology, emphasizing the role of heart valves in maintaining proper blood flow. Utilize visual aids, such as diagrams, animations, and 3D models, to illustrate normal valve function and the pathophysiology of common conditions like stenosis and regurgitation. Incorporate case studies and real-world scenarios to demonstrate symptom recognition, diagnostic techniques (e.g., auscultation, echocardiography), and nursing interventions, such as medication management and patient education. Encourage hands-on practice through simulation labs to reinforce assessment skills and critical thinking. Finally, emphasize the importance of holistic patient care, including emotional support and long-term management strategies, to prepare students for compassionate and effective practice in diverse healthcare settings.
Explore related products






What You'll Learn
- Understanding Valvular Anatomy: Basics of heart valves, their structure, and normal function
- Types of Valvular Diseases: Stenosis, regurgitation, causes, and affected valves
- Clinical Manifestations: Symptoms, physical exam findings, and diagnostic clues
- Diagnostic Tools: Echocardiography, ECG, and other imaging techniques explained
- Nursing Care & Management: Patient education, medications, and post-op care strategies
![]()
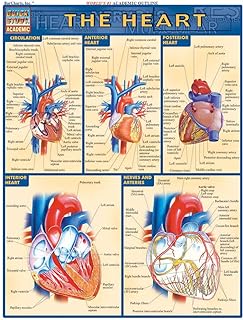
Understanding Valvular Anatomy: Basics of heart valves, their structure, and normal function
The human heart is a marvel of engineering, with four valves acting as precision gates, ensuring unidirectional blood flow. Understanding their anatomy is foundational for grasping valvular diseases. The mitral and tricuspid valves, situated between the atria and ventricles, are composed of leaflets (two for the mitral, three for the tricuspid) and chordae tendineae, which prevent prolapse during systole. The aortic and pulmonary valves, positioned at the ventricular outflows, are trileaflet structures that open under pressure to allow blood ejection. Each valve’s unique design reflects its function: the mitral valve’s larger surface area accommodates higher volumes, while the aortic valve’s thicker leaflets withstand systemic pressures.
Teaching valvular anatomy effectively requires a multimodal approach. Begin with 3D models or animations to illustrate leaflet movement during the cardiac cycle. Pair this with auscultation simulations, allowing students to correlate normal valve sounds (e.g., the “lub-dub” of mitral and aortic closure) with anatomical function. Caution against oversimplification: emphasize that even minor structural deviations, like thickened leaflets or fused commissures, can disrupt flow dynamics. For instance, a bicuspid aortic valve, present in 1-2% of the population, predisposes to stenosis due to reduced leaflet flexibility.
A comparative analysis of valve structures highlights their interdependence. The mitral valve’s chordae attach to the papillary muscles, which, if weakened (e.g., post-MI), can cause regurgitation. In contrast, the aortic valve’s direct exposure to systemic pressure makes it prone to calcification in older adults. Encourage students to draw parallels between anatomy and pathophysiology: a stenotic tricuspid valve increases right atrial pressure, leading to hepatic congestion and ascites. This approach bridges theory and clinical practice, fostering critical thinking.
Practical tips for teaching include using mnemonic devices, such as “MAP” (Mitral-Aortic-Pulmonary) to recall valve positions, or “LARP” (Left Atrium-Right Pulmonary) for blood flow direction. Incorporate case studies of patients with congenital anomalies, like Ebstein’s anomaly (malpositioned tricuspid valve), to demonstrate real-world implications. For hands-on learning, have students palpate carotid pulses while listening to heart sounds, reinforcing the link between valve function and peripheral findings.
In conclusion, mastering valvular anatomy is not about memorization but understanding the interplay of structure and function. By combining visual aids, simulations, and clinical correlations, educators can demystify complex concepts. Equip students with the tools to recognize deviations from normal anatomy, as this forms the bedrock for diagnosing and managing valvular diseases effectively.
Securing Your Student Teaching Work Site: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Types of Valvular Diseases: Stenosis, regurgitation, causes, and affected valves
Valvular diseases manifest primarily as stenosis or regurgitation, each with distinct pathophysiological mechanisms and clinical implications. Stenosis occurs when a valve narrows, obstructing blood flow. For instance, aortic stenosis limits left ventricular outflow, forcing the heart to work harder. Nursing students should visualize this as a partially closed door, restricting movement. Regurgitation, in contrast, involves valve incompetence, allowing blood to leak backward. Mitral regurgitation, for example, causes blood to flow from the left ventricle back into the left atrium during systole. Analogize this to a leaky faucet, wasting effort and resources. Understanding these differences is foundational for assessing symptoms, diagnostic findings, and interventions.
Teaching the causes and affected valves requires a systematic approach. Rheumatic fever, a sequela of untreated streptococcal infection, remains a leading cause of mitral stenosis globally, particularly in low-resource settings. Age-related calcification, however, is the primary driver of aortic stenosis in older adults (>65 years). For regurgitation, degenerative changes (e.g., myxomatous degeneration) commonly affect the mitral valve, while infective endocarditis can destroy any valve, often the aortic. Instruct students to correlate patient history (e.g., prior strep throat, IV drug use) with valve involvement. Practical tip: Use diagrams or 3D heart models to demonstrate how each valve’s anatomy predisposes it to specific diseases.
When explaining clinical manifestations, emphasize how stenosis and regurgitation differ. Stenosis typically presents with exertional symptoms (e.g., dyspnea, angina) due to reduced cardiac output, while regurgitation may cause volume overload symptoms (e.g., fatigue, orthopnea). For aortic stenosis, the classic triad is chest pain, syncope, and heart failure. Mitral regurgitation often produces a high-pitched, holosystolic murmur heard best at the apex. Caution students to avoid misdiagnosis: murmurs alone are insufficient for diagnosis; echocardiography is essential. Dosage note: Patients with severe stenosis may require careful fluid management to avoid precipitating heart failure.
To reinforce learning, employ comparative case studies. Present a 70-year-old with gradual dyspnea and a harsh, crescendo-decrescendo murmur (aortic stenosis) alongside a 40-year-old with acute rheumatic fever history and an opening snap (mitral stenosis). Ask students to identify the affected valve, underlying cause, and expected hemodynamic changes. Follow with a regurgitation case: a 55-year-old with flail mitral leaflet and pulsations in the apex. This approach bridges theory and practice, fostering critical thinking. Takeaway: Valvular diseases are not one-size-fits-all; precise diagnosis dictates management, from medical therapy to surgical intervention.
Finally, integrate practical tips for nursing care. Patients with stenosis require monitoring for syncope or angina, while those with regurgitation need assessment for volume overload (e.g., jugular venous distension, S3 gallop). Teach students to educate patients on endocarditis prophylaxis (e.g., dental hygiene, antibiotic coverage for procedures) and activity restrictions in severe cases. For post-operative patients, emphasize monitoring for bleeding (due to anticoagulants) and valve dysfunction. Example: A mechanical aortic valve replacement patient needs lifelong warfarin with an INR target of 2.0–3.0. Conclusion: Mastery of valvular disease types empowers nurses to deliver targeted, patient-centered care.
Creative Strategies for Teaching the Alphabet in Special Education Classrooms
You may want to see also
Explore related products






![]()
Clinical Manifestations: Symptoms, physical exam findings, and diagnostic clues
Valvular heart diseases present a unique challenge in clinical practice due to their varied and often subtle manifestations. Teaching nursing students to recognize these signs requires a structured approach that bridges theoretical knowledge with practical skills. Begin by emphasizing that symptoms are the patient’s narrative, while physical exam findings and diagnostic clues are the nurse’s tools to validate and deepen that story. For instance, a patient with aortic stenosis may describe exertional dyspnea or angina, but it’s the harsh, crescendo-decrescendo murmur heard at the right second intercostal space that confirms the diagnosis. This interplay between subjective and objective data is critical for early detection and intervention.
Instruct students to think systematically when assessing patients with suspected valvular disease. Start with symptoms: dyspnea, fatigue, and edema are common across conditions but vary in onset and severity. Mitral regurgitation, for example, often presents with gradual onset of orthopnea and paroxysmal nocturnal dyspnea, whereas aortic regurgitation may cause exertional dyspnea and a wide pulse pressure. Next, guide them to perform a focused physical exam, highlighting key findings like jugular venous distension in tricuspid regurgitation or a diastolic murmur in mitral stenosis. Teach them to use the diaphragm of the stethoscope for low-pitched murmurs and the bell for high-pitched sounds, ensuring they don’t miss critical clues.
Persuade students to view diagnostic tests as extensions of their clinical reasoning. An echocardiogram is the gold standard for confirming valvular disease, but chest X-rays and ECGs provide valuable preliminary insights. For instance, left atrial enlargement on a chest X-ray suggests mitral stenosis, while left ventricular hypertrophy on an ECG may indicate aortic stenosis. Encourage them to correlate these findings with the patient’s history and physical exam, reinforcing the importance of a holistic approach. For example, a patient with a history of rheumatic fever and a heart murmur should prompt suspicion of mitral valve involvement, guiding the need for further imaging.
Compare and contrast the manifestations of different valvular diseases to sharpen diagnostic acumen. Mitral stenosis and aortic stenosis both cause dyspnea, but the former is associated with a low-pitched diastolic rumble, while the latter produces a high-pitched systolic murmur. Similarly, aortic regurgitation and mitral regurgitation may both present with a wide pulse pressure, but the former has a characteristic “water hammer” pulse, and the latter often includes a holosystolic murmur heard at the apex. This comparative approach helps students differentiate between conditions with overlapping symptoms, reducing diagnostic errors.
Finally, provide practical tips to enhance learning retention. Use mnemonic devices like “AUNT MARY” (Aortic stenosis: Angina, Unemia, Near syncope, Tiredness; Mitral regurgitation: Murmur, Apex, Radiating, Young patients) to help students recall key features. Incorporate simulation exercises where students practice auscultating murmurs on mannequins or peers, reinforcing their ability to identify subtle differences. Encourage them to document findings systematically, using phrases like “3/6 holosystolic murmur at the apex radiating to the axilla” to ensure clarity and precision. By combining theoretical knowledge with hands-on practice, nursing students can develop the confidence and competence needed to manage valvular diseases effectively.
Inspiring Young Writers: Strategies for Teachers to Motivate Student Writing
You may want to see also
Explore related products






![]()
Diagnostic Tools: Echocardiography, ECG, and other imaging techniques explained
Echocardiography stands as the cornerstone in diagnosing valvular diseases, offering a non-invasive window into the heart's structure and function. This imaging technique uses ultrasound waves to create real-time images of the heart valves, allowing nurses to visualize leaflet motion, stenosis, regurgitation, and chamber size. For instance, in mitral stenosis, echocardiography reveals thickened, immobile leaflets and a domed appearance of the atrial side of the valve. Teaching students to interpret these findings requires hands-on practice with annotated images and case studies. Emphasize the importance of Doppler studies, which quantify blood flow velocity and pressure gradients, critical for grading disease severity. For example, a mean gradient of >10 mmHg in aortic stenosis indicates severe disease, necessitating surgical intervention.
While echocardiography provides detailed anatomical insights, the electrocardiogram (ECG) serves as a complementary tool, highlighting the electrical consequences of valvular dysfunction. Left-sided valve diseases, such as aortic stenosis or mitral regurgitation, often manifest as left ventricular hypertrophy (LVH) on ECG, characterized by increased QRS voltage or ST-T wave changes. Nursing students should learn to recognize these patterns, understanding that LVH reflects the heart’s compensatory response to increased workload. However, ECG alone is insufficient for diagnosis; it merely flags the need for further imaging. Caution students against over-interpreting ECG findings without correlating them with echocardiographic data. For instance, LVH on ECG in a patient with aortic stenosis confirms the hemodynamic impact of the valve lesion.
Beyond echocardiography and ECG, advanced imaging techniques like cardiac MRI and CT angiography play specialized roles in valvular disease assessment. Cardiac MRI excels in quantifying valve regurgitation volumes and assessing myocardial fibrosis, particularly in patients with rheumatic heart disease or infective endocarditis. CT angiography, with its high spatial resolution, is invaluable for evaluating calcification patterns in aortic stenosis or planning transcatheter valve interventions. When teaching these modalities, focus on their unique strengths and limitations. For example, MRI’s lack of radiation makes it ideal for younger patients, while CT’s rapid acquisition is advantageous in acute settings. Encourage students to consider patient factors like renal function (contrast use) and claustrophobia when selecting imaging modalities.
Integrating these diagnostic tools into clinical practice requires a systematic approach. Start by teaching students to correlate symptoms (e.g., dyspnea, chest pain) with initial ECG findings, then guide them to use echocardiography for definitive diagnosis. For complex cases, such as prosthetic valve dysfunction, introduce advanced imaging as a problem-solving step. Practical tips include ensuring patients are in optimal positions for echocardiography (left lateral decubitus) and explaining procedures clearly to reduce anxiety. Reinforce the importance of multidisciplinary collaboration, as cardiologists, radiologists, and surgeons rely on these images for treatment planning. By mastering these tools, nursing students become essential contributors to the diagnostic and care teams.
Homeschooling Check-Ins: How Often Should Students Connect with Teachers?
You may want to see also
Explore related products





![]()
Nursing Care & Management: Patient education, medications, and post-op care strategies
Effective nursing care for patients with valvular diseases hinges on a triad of patient education, precise medication management, and meticulous post-operative care. Begin by empowering patients through education, as informed individuals are more likely to adhere to treatment plans. Teach them about their specific valve condition—whether it’s stenosis, regurgitation, or a combination—and explain how it affects blood flow and overall health. Use visual aids like diagrams or animations to illustrate normal vs. abnormal valve function, and emphasize symptoms such as shortness of breath, fatigue, or chest pain that warrant immediate attention. For instance, a patient with aortic stenosis should understand the importance of monitoring for syncope or angina, which could signal disease progression.
Medication management is critical in stabilizing patients pre- and post-operatively. Diuretics like furosemide (20–40 mg daily) are often prescribed to manage fluid overload in patients with valve regurgitation, but caution must be taken to monitor electrolytes, especially potassium levels. For patients with atrial fibrillation secondary to valvular disease, anticoagulants such as warfarin (target INR 2.0–3.0) or direct oral anticoagulants (DOACs) are essential to prevent thromboembolic events. Nursing students should learn to educate patients about medication adherence, potential side effects, and the importance of regular follow-ups. For example, emphasize that missing doses of warfarin can increase stroke risk, while over-anticoagulation can lead to bleeding complications.
Post-operative care is a high-stakes phase requiring vigilance and proactive management. After valve replacement or repair surgery, monitor for signs of bleeding, infection, or thrombus formation. Patients with mechanical valves require lifelong anticoagulation, while those with bioprosthetic valves may need it temporarily. Teach students to assess incision sites for erythema, warmth, or drainage, and to monitor vital signs for irregularities. Pain management is also crucial; administer opioids judiciously, balancing relief with the risk of respiratory depression, especially in elderly patients. Encourage early ambulation to prevent complications like pneumonia or deep vein thrombosis, but ensure patients understand their activity limits, particularly in the first 6–8 weeks post-surgery.
Finally, integrate a holistic approach by addressing psychological and lifestyle adjustments. Patients may experience anxiety or depression post-surgery, so screen for these symptoms and provide resources for mental health support. Educate on heart-healthy diets low in sodium and saturated fats, and stress the importance of regular exercise within prescribed limits. For example, a 60-year-old patient with a new aortic valve may safely engage in walking or swimming but should avoid strenuous activities like weightlifting. By combining technical knowledge with compassionate care, nursing students can become adept at managing valvular disease patients across the continuum of care.
Teaching Logic Problems to Elementary Students: Fun and Effective Strategies
You may want to see also
Frequently asked questions
The key objectives include understanding the anatomy and function of heart valves, recognizing symptoms and risk factors of valvular diseases, learning diagnostic methods (e.g., echocardiography), and mastering nursing interventions for patient care and education.
Use visual aids like diagrams, animations, and models to illustrate valve anatomy and dysfunction. Relate concepts to real-life scenarios and encourage hands-on practice with auscultation and patient simulations.
Focus on aortic stenosis, mitral regurgitation, mitral stenosis, and tricuspid regurgitation, as these are the most prevalent and clinically significant conditions.
Teach them to identify murmur characteristics (timing, location, intensity, and quality) and correlate them with specific valve disorders. Use audio recordings and practice sessions with stethoscopes for better retention.
Emphasize the importance of teaching patients about symptom recognition, medication adherence, lifestyle modifications, and follow-up care. Role-playing scenarios can help students practice effective communication skills.